
Photo-based remote PD measurement captures pupillary distance within +/-0.5 to 1mm accuracy from a single smartphone photograph, reducing measurement time from 5-10 minutes to under 60 seconds. According to clinical research published in PMC, leading smartphone applications achieve a mean absolute error of 0.51mm, comparable to digital pupillometers. For optical retailers, this means enabling online sales, recovering 15-20 staff hours per week, and serving patients outside your geographic area, all without purchasing dedicated equipment.
Pupillary distance (PD) is the distance in millimeters between the centers of both pupils, measured when looking straight ahead at a distant object. Accurate PD ensures the optical center of each lens aligns with the wearer’s pupil, preventing eyestrain and blurred vision. The ISO 13666:2019 standard defines it as “the distance between the centres of the pupils when the eyes are fixating an object at an infinite distance in the straight-ahead position.”
4 Clinical and Business Benefits of Remote PD Measurement
Eliminating Geographic Barriers for Rural and Mobility-Limited Patients
Remote PD measurement expands the addressable market for optical retailers by removing geographic and accessibility constraints. Patients in rural areas, those with mobility challenges, or individuals in regions with limited optical services can receive accurate PD measurements without traveling to a physical location.
The clinical standard for acceptable PD measurement accuracy is +/-2mm for single vision lenses and +/-1mm for progressive lenses, according to ANSI Z80.1 ophthalmic standards. Photo-based measurement systems consistently achieve accuracy within these tolerances.
Key accessibility advantages:
- Patients can submit measurements from any location with smartphone access
- Eliminates transportation barriers for elderly or mobility-impaired individuals
- Extends service to underserved geographic markets
- Enables asynchronous service delivery (measurements processed outside business hours)
The AOA’s telemedicine guidelines emphasize that the standard of care must remain consistent regardless of whether services are delivered in-person or remotely, making accuracy validation critical for remote measurement implementations.
Reducing Measurement Time from 10 Minutes to 60 Seconds
Traditional manual PD measurement using a millimeter ruler, the approach detailed in our guide on how to measure PD at home, typically requires 5-10 minutes per patient when performed according to proper clinical protocols. Photo-based PD measurement systems reduce this to 30-60 seconds total, including image capture, automated processing, and verification.
Workflow impact analysis:
| Measurement Method | Time per Patient | Accuracy Range | Staff Training Required |
|---|---|---|---|
| Manual ruler | 5-10 minutes | +/-2mm typical | 2-4 hours |
| Digital pupillometer | 2-3 minutes | +/-0.5mm | 1-2 hours |
| Photo-based (remote) | 30-60 seconds | +/-0.5-1mm | 1-2 hours |
The time savings compound across use cases: in-store staff can serve multiple customers simultaneously, online orders eliminate appointment scheduling overhead, and stored measurements enable instant reorders without requiring patients to return.
Research on smartphone application accuracy for IPD measurement demonstrates that applications using reference-object calibration methods achieve accuracy comparable to digital pupillometers while requiring significantly less time and no specialized equipment beyond a smartphone camera.
ROI Analysis: How Remote PD Cuts Operating Costs by 30-40%
Based on Optogrid’s internal analysis of customer data across optical practices of varying sizes, remote PD implementation typically creates 30-40% cost savings across measurement-related expenses.
Direct cost savings (annual) for a mid-sized practice:
- Labor efficiency: 15-20 staff hours/week recovered at $25/hour = $19,500-26,000
- Equipment costs: Eliminate $500-2,000 digital pupillometer purchases or replacements
- Reduced errors: 40% reduction in remake/adjustment costs (typical practice spends $8,000-12,000/year on remakes)
Revenue expansion opportunities:
- Online sales channel: New revenue averaging $30,000-80,000 annually for established practices
- Extended service hours: After-hours measurement submission enables 24/7 order intake
- Geographic expansion: Serve customers outside your primary service area
Total annual impact: $58,000-120,000 for a typical practice processing 50-100 eyewear orders monthly (Optogrid internal analysis).
The global eyewear market is projected to reach $335.90 billion by 2030, with online channels growing at 12% CAGR (compound annual growth rate). Practices implementing remote measurement capabilities position themselves to capture a growing share of online demand.
For SaaS (software as a service) solutions like Optogrid, which captures binocular PD, monocular PD, and segment height from a single patient photograph via a browser link with no app download required, the typical payback period is 2-4 months based on labor savings alone.
Competitive Positioning: Why Early Adopters Capture More Online Sales
The e-commerce eyewear market is projected to reach $77.71 billion by 2035, representing 20-25% of total eyewear sales. Practices without remote measurement capabilities are effectively locked out of this segment.
Competitive positioning advantages:
- Market differentiation: Remote PD capability serves as a clear value proposition in customer acquisition
- Customer retention: Convenience features reduce defection to online-only competitors
- Price premium justification: Technology-enabled service supports premium pricing versus pure-discount competitors
The 2024 FTC Eyeglass Rule update explicitly encourages prescribers to provide PD measurements to patients who request them. Only Kansas, Massachusetts, Alaska, and New Mexico currently mandate PD inclusion on prescriptions, though this may expand as online purchasing grows.
Understanding Remote PD Measurement Technology
How Computer Vision Algorithms Detect Pupil Centers
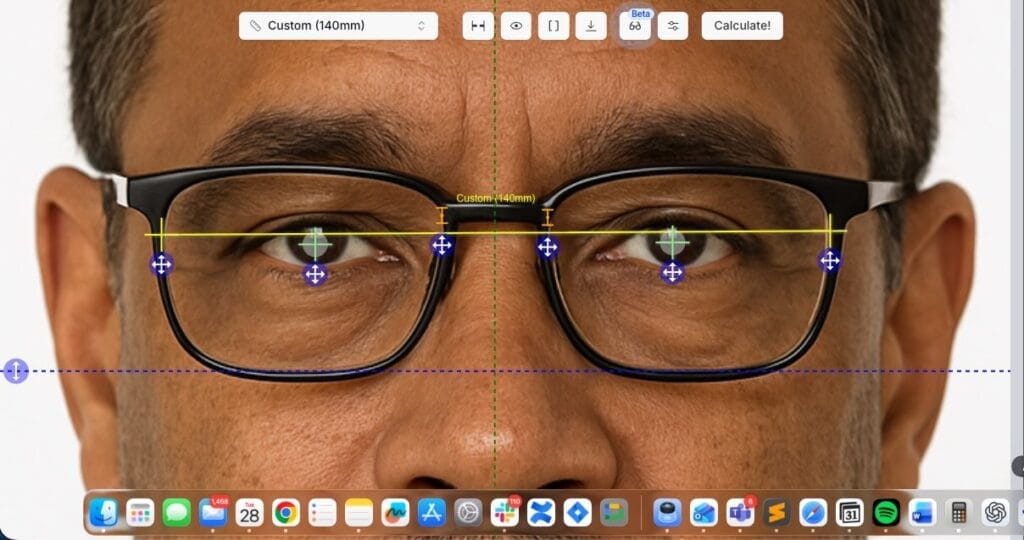
Modern remote PD measurement systems use machine learning-trained computer vision algorithms to identify facial landmarks with sub-millimeter precision. The process follows these technical steps:
- Facial landmark detection: The algorithm identifies 68-194 facial landmarks depending on the model, including eye corners, pupil centers, and nose bridge
- Pupil center localization: Specialized algorithms detect the geometric center of each pupil by analyzing contrast patterns between the pupil (dark) and iris/sclera (lighter)
- Scale calibration: A reference object of known dimensions (credit card, government ID, or calibrated marker) establishes the pixels-to-millimeters conversion ratio
- Distance calculation: With scale established and pupil centers identified, the system calculates linear distance between pupil centers in millimeters
- Quality validation: Algorithms assess image quality factors (lighting, blur, head angle) and flag measurements that fail quality thresholds
These systems use convolutional neural networks (CNNs), a type of deep learning model trained on millions of faces that can identify precise facial landmarks with greater than 95% accuracy, even under variable lighting conditions.
According to research on smartphone pupillometer feasibility, photo-based system accuracy depends critically on proper calibration methods and image quality controls. Systems implementing multi-point calibration demonstrate accuracy within +/-0.5-1mm of clinical-grade pupillometers.
Quality Factors Affecting Remote Measurement Accuracy
Photo-based PD measurement accuracy depends on several controllable factors:
- Lighting: Even, frontal lighting produces clear pupil boundaries; side lighting or backlighting reduces accuracy
- Camera resolution: Minimum 8MP recommended; 12MP+ ideal for consistent sub-millimeter accuracy
- Head positioning: Face must be perpendicular to camera; head tilt greater than 5 degrees degrades accuracy
- Focus quality: Sharp focus on eyes essential; blur increases center-detection error
- Reference object placement: Credit card or calibration card must be in same plane as eyes
- Eye gaze direction: Eyes looking directly at camera; off-axis gaze creates parallax error
Modern systems like Optogrid implement automated quality checks that reject images failing these criteria before processing, ensuring only high-quality measurements reach the practitioner.
When Remote PD Measurement Is and Is Not Appropriate
Remote PD measurement serves many use cases effectively, but understanding its limitations ensures appropriate clinical application.
Appropriate Use Cases
- Standard prescription strength: -8.00D to +4.00D sphere, up to -4.00D cylinder
- Single vision lenses: Distance or reading glasses without progressive or bifocal requirements
- Progressive lenses (monocular PD available): When dual/monocular PD measurements are captured separately for each eye
- Frame reorders: Patient ordering replacement glasses in same frame style
- Sunglasses and fashion eyewear: Non-prescription or standard prescriptions
Situations Requiring In-Person Measurement
- High prescription strengths: Greater than +/-8.00D sphere or greater than 4.00D cylinder where +/-0.5mm accuracy is critical. At these powers, vertex distance compensation also becomes critical, since even a 2mm change in fitting distance meaningfully shifts the effective power at the eye.
- Prismatic corrections: Prescriptions with prism require precise PD measurement and fitting height
- Complex progressive designs: Short-corridor progressives or occupational lenses with specific fitting requirements
- Pediatric patients: Children under 10-12 years may have difficulty following photography instructions. For guidance on working with younger patients, see measuring PD in children, which covers reference norms by age and practical tips for cooperative capture.
- Post-surgical patients: Recent cataract, refractive, or other ocular surgeries require in-person evaluation
- Significant anisometropia (where the two eyes have substantially different refractive power, greater than 3.00D difference between eyes): requires careful in-person PD verification
For detailed fitting protocols for high-Rx patients and specialized lens designs, see our clinical guide to prescription lens fitting for special conditions.
The AOA telemedicine guidelines emphasize that practitioners must refer patients for in-person care when clinically appropriate. The same principle applies to measurement technology selection.
Implementation Roadmap: Adding Remote PD to Your Practice
Phase 1: Technology Selection and Integration (Weeks 1-2)
Evaluate solutions on these criteria:
- Accuracy validation: Request data comparing the system to clinical-grade pupillometers
- Integration capabilities: API availability, compatibility with existing practice management systems
- User experience: Patient-facing interface simplicity (mobile-friendly, clear instructions)
- Quality controls: Automated image quality assessment and rejection protocols
Optogrid offers a web-based measurement solution requiring no app download. It integrates via link sharing or website embedding and captures binocular PD, monocular PD, and segment height from a single photograph. Opticians can send a patient link directly to the patient’s phone so they complete the capture at home before the order is placed.
Phase 2: Staff Training and Protocol Development (Weeks 2-3)
Training takes 1-2 hours total, covering: how the system works, how to evaluate measurement quality, when remote measurement is appropriate vs. when in-person is required, and common troubleshooting (poor lighting, incorrect reference object, head angle problems).
Document clinical protocols defining appropriate use cases, quality thresholds, and re-measurement procedures.
Phase 3: Workflow Integration and Testing (Weeks 3-4)
Integrate remote PD into four workflow points: in-store orders (as a time-saving option), online orders (in e-commerce checkout flow), follow-up orders (using stored measurements), and remote consultations (combined with telehealth where legally permitted).
Conduct parallel measurements (remote plus in-person) for the first 20-30 patients to validate accuracy in your environment.
Phase 4: Marketing and Patient Education (Week 4+)
Update your website with remote measurement capability, create patient education materials explaining how to take quality photos, and promote online ordering through email, social media, and in-store signage.
Early adopter practices typically see 15-25% of eligible patients choose remote measurement within the first 3 months, growing to 40-50% adoption by month 6.
For step-by-step implementation guidance specific to Optogrid, see our measurement guide covering PD, dual PD, and segment height.
Data-Driven Insights: What 14,900+ Remote PD Measurements Reveal
Optogrid’s analysis of 14,904 PD measurements captured between January-June 2025 reveals clinically relevant patterns:
- Mean binocular PD: 63.2mm (closely matching published anthropometric data)
- Standard deviation: 3.4mm (indicating typical population variation)
- Gender differences: Males average 64.1mm; females average 62.3mm (1.8mm difference)
- Measurement precision: 94% of measurements fall within expected population distribution (40-90mm range)
- Outlier detection: 6% flagged as potential errors or quality issues
This data enables statistical quality controls. When a remote measurement falls outside expected ranges (more than 3 standard deviations from population mean), the system flags it for manual review. A measurement of 52mm for an adult male or 72mm for an adult female should trigger verification, as these fall well outside typical ranges.
Progressive Lens Fitting: Segment Height and Remote Measurement
Remote PD technology has expanded beyond basic binocular PD to include segment height (SH), the vertical distance from the bottom of the lens to the pupil center when the patient is in primary gaze. Incorrect SH measurements can result in narrow or unusable intermediate/near zones in progressive lenses.
Remote SH measurement considerations:
- Photo-based systems capture SH simultaneously with PD when patients photograph themselves wearing their chosen frame
- Accuracy requirements for SH are similar to PD: +/-1mm acceptable for most progressive designs
- Reference object calibration establishes scale for both horizontal (PD) and vertical (SH) measurements
- Patients must photograph themselves with the frame at proper wearing position
For comprehensive guidance on segment height measurement, including typical SH ranges and common fitting mistakes, see our segment height fitting guide for progressive lenses.
Modern progressive lens designs also require pantoscopic tilt (frame angle relative to vertical, typically 8-12 degrees) and vertex distance (distance from back lens surface to cornea, typically 12-14mm). Remote capture of these parameters remains technically challenging and typically requires in-person measurement.
For additional context on digital PD measurement evolution, see our article on the rise of the digital PD ruler.
Frequently Asked Questions About Remote PD Measurement
Is remote PD measurement as accurate as in-person measurement?
For most prescription types, yes. Peer-reviewed research shows that leading smartphone PD applications achieve a mean absolute error of 0.51mm, comparable to digital pupillometers. This accuracy meets ANSI Z80.1 tolerances for single vision and most progressive lens designs. For very high prescriptions (greater than +/-8.00D sphere) or prism corrections, in-person measurement with a digital pupillometer is preferable.
What equipment do I need for remote PD measurement?
Patients need only a smartphone with a camera (8MP or higher) and a reference object such as a credit card or government ID. No specialized equipment is required. Practice-side, you need a computer or tablet with internet access to review measurements. SaaS-based solutions like Optogrid operate through web browsers, eliminating software installation or hardware purchases.
How much time does remote PD measurement save per patient?
Remote PD reduces measurement time from 5-10 minutes (manual ruler) to 30-60 seconds, a 90% reduction. For a practice processing 50 measurements weekly, that recovers 4-8 staff hours per week. Stored measurements also enable instant reorders without requiring patients to return.
What are the legal requirements for remote PD measurement?
Federal regulations do not restrict remote PD measurement. The 2024 FTC Eyeglass Rule update encourages prescribers to provide PD to patients upon request but does not mandate it. Only Kansas, Massachusetts, Alaska, and New Mexico require PD on prescriptions. The primary compliance consideration is HIPAA: patient photographs are protected health information and must be handled securely.
What accuracy range do photo-based PD systems achieve?
Photo-based systems typically achieve +/-0.5-1mm accuracy with proper quality controls, according to published clinical research. This meets ANSI Z80.1 standards specifying +/-2mm tolerance for single vision and +/-1mm for progressives. Accuracy depends on lighting quality, camera resolution (12MP+ recommended), head positioning, and reference object placement.
Can remote PD measurement work for children?
Remote PD can work for children aged 10-12 and older who can follow photography instructions. Younger children typically require in-person measurement due to difficulty with head positioning and gaze direction. Pediatric PD averages are also smaller (50-55mm for ages 6-10), which demands careful quality control to maintain accuracy at these measurements.
How does remote PD integrate with practice management software?
Most modern solutions offer multiple integration options: API integration for automated data transfer, web-based dashboard access, CSV export/import, or manual data entry. Optogrid provides API integration for practices with development resources and a web-based dashboard for manual workflows. API connections that auto-populate PD measurements into your practice management system eliminate transcription errors.
What is the ROI timeline for implementing remote PD measurement?
Most practices achieve positive ROI within 2-4 months based on labor savings alone. A mid-sized practice (50-100 orders monthly) using a SaaS solution can expect $19,500-26,000 in recovered labor costs annually, plus $3,000-5,000 in reduced remake costs. Annual SaaS subscription costs typically range from $1,200-3,000, making the payback period short even before accounting for online sales revenue.
Three Decision Criteria for Evaluating Remote PD Technology
When selecting a remote PD measurement solution, prioritize these factors:
- Clinical accuracy validation. Request published or internal accuracy data comparing the system to digital pupillometers across prescription types. Systems achieving +/-0.5-1mm with automated quality rejection are the current benchmark.
- Integration friction. Browser-based solutions that require no app download minimize patient drop-off. Evaluate API compatibility with your practice management system and whether the solution supports both PD and segment height capture.
- Regulatory readiness. Confirm HIPAA compliance (Business Associate Agreement required), data encryption in transit and at rest, and compliant data retention policies. As state PD-on-prescription mandates expand beyond the current four states, practices with established remote measurement workflows will adapt faster.
Remote PD measurement is moving toward integration with virtual try-on platforms and full frame fitting parameter capture (pantoscopic tilt, vertex distance, wrap angle). Practices that build remote measurement into their workflows now will be positioned to adopt these capabilities as they mature.
Optical practices ready to add remote PD can explore how to measure PD, dual PD, and segment height with Optogrid, a browser-based solution requiring no equipment purchase or app download.
Sources
Research and industry sources cited in this article:
- Comparing the Effectiveness of Smartphone Applications in the Measurement of Interpupillary Distance – PMC
- ISO 13666:2019 – Ophthalmic Optics Spectacle Lenses Vocabulary – International Organization for Standardization
- ANSI Z80.1-2020 – Ophthalmics Prescription Ophthalmic Lenses – American National Standards Institute
- AOA Position Statement on Telemedicine in Optometry – American Optometric Association, revised 2025
- Federal Register: Ophthalmic Practice Rules (Eyeglass Rule) – Federal Trade Commission, July 2024
- Eyewear Market Size, Share & Trends – Grand View Research
- E-Commerce Eyewear Market Growth Report – Market Research Future
- Feasibility Study of a Smartphone Pupillometer – PubMed
- Pupil Distance Average 2025: Data from 14,900+ Measurements – Optogrid

I grew up inside an optical shop. My mother likes to tell how, as a kid, I would watch eyeglasses being assembled, play with the tools, and draw on the back of service order slips. The family business taught me early what a precise measurement and work done right are worth.
I went on to spend more than twenty years as a software engineer, always keeping an eye on the optical world. Optogrid was born where the two meet: digital measurement technology (pupillary distance and fitting heights) built by someone who knows the dispensing counter from the inside.